Date: Monday, 18 September 2023
Authors Smret TM , Weldegergis RK, Achila OO , Tekle AM
Received 20 June 2023
Accepted for publication 1 September 2023
Published 18 September 2023 Volume 2023:15 Pages 213—224
DOI https://doi.org/10.2147/OPTO.S421366
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Mr Simon Berry
Tsige Mnasie Smret,1 Rahel Kesete Weldegergis,2 Oliver Okoth Achila,3 Alexander Mulugeta Tekle4
1Department of Optometry, Biet Mekae Community Hospital, Asmara, Eritrea; 2Department of Optometry, Vision Express Eye Care Clinic, Addis Ababa, Ethiopia; 3Department of Clinical Laboratory Science, Orotta College of Medicine and Health Sciences, Asmara, Eritrea; 4Department of Optometry, Hazhaz Zonal Referral Hospital, Asmara, Eritrea
Correspondence: Tsige Mnasie Smret; Rahel Kesete Weldegergis, Email tsigemnasie@gmail.com; rachelkesete@gmal.com
Background: Presbyopia is an age-related progressive decrease of near vision, corrected by near addition glasses. These age-appropriate glasses, however, vary across different geographical locations and populations. But there is no existing information on the age-based addition for Asmara and high number of uncorrected presbyopes, so this study determined the required age-based addition for the presbyopes in Asmara.
Methods: A cross-sectional study was conducted on patients aged 35– 60 years who visited all eye centers in the city. Patients with best-corrected visual acuity in both eyes better than 6/9 were included in the study. Near add was calculated using Monocular Estimation Method (MEM) and amplitude of accommodation results. Data entry and analysis were performed using Statistical Package for the Social Sciences v. 20.
Results: This study included 1310 participants of whom 48.5% were females and 51.5% were males. The prevalence of presbyopia was found to be 74.1% out of which 44% were females. There were 35.6% of the participants with a previous prescription for glasses, though only 24% of the participants presented with glasses on. Among the different occupational categories, laborers were the ones who had the highest number of presbyopes (79.5%), office workers (73%), and housewives (68.7%). The mean age of those with presbyopes was 49.5 ± 5.8 years. Multivariable analysis performed for presbyopia showed that older age and female sex were associated with a higher likelihood of presbyopia (< 0.005). An addition table was prepared separately for males and females. On post-hoc tests, no significant association was found between the given and the different refractive status.
Conclusion: The study showed that there is a high level of uncorrected presbyopes in the city, so the availability of refraction sites and glasses accessibility needs to increase. The near addition demand for this population varies from the previously stated amount in other countries. Therefore, guidelines specifically prepared for a society are necessary.
Keywords: presbyopia, near addition glasses, Asmara, amplitude of accommodation
According to Global Burden of Disease in 2020 presbyopia was estimated to be the cause of vision impairment in 510 million people of whom 280 million were females.1 It was estimated to affect 1.8 billion people around the globe in 2015, with an unmet need of 45% globally.2 The global productivity loss of working-age group (>50 years) was estimated at US $11 billion annually in 2011 because of uncorrected and under-corrected presbyopia.3 As life expectancy and demand for clear vision are increasing, presbyopia poses a significant public health concern.
 | Figure 1 Near addition distribution across the age groups. Notes: Vertical line = near addition. Horizontal line = age. Figure 1 illustrates the result of post hoc tests which were run on the addition across the age groups and the result showed there was a significant difference in the addition across the different age groups with a p-value of <0.001. |
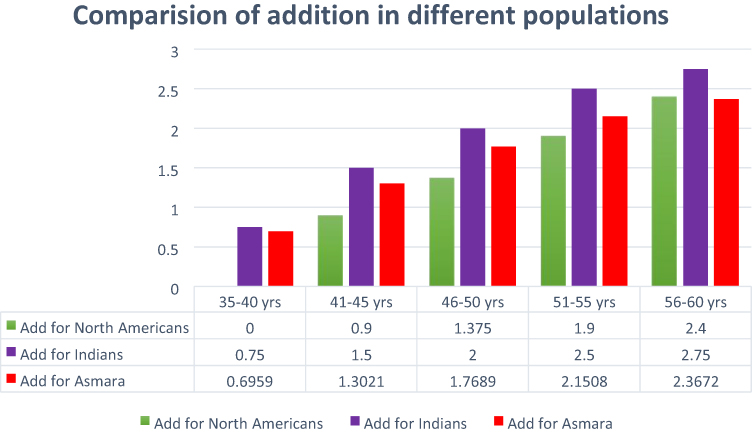 | Figure 2 Comparison of the addition of different populations. Notes: Vertical line = near addition values. Horizontal line = age groups. The variation in addition for these populations is illustrated in Figure 2. |
Various studies have been conducted in different countries on the prevalence of presbyopia and its impact on quality of life of their individuals. In population based cross-sectional studies conducted in Japan and Kenya the prevalence of presbyopia was 43.8% and 25.1% in those above 30 years of age,4,5 in Haryana, India in those above 35 years there was prevalence of 42.9%.6 A study conducted in Nigerian school teachers in the age range of 30–61 years had a prevalence of 81.3%7 with 38.5% of them without correction; a similar study conducted in Gondar, Ethiopia in school teachers found a prevalence of presbyopia of 68.7%. In Ghana it was 68.1% with an unmet need of 54.1%.7–9
Presbyopia is an age-related visual impairment that results from the gradual decrease in accommodation expected with age. It affects quality of vision and quality of life (QoL).10 It comes from the gradual thickening and loss of viscoelasticity of the crystalline lens. Blurred vision and asthenopia at near working distance are hallmarks of presbyopia.10,11 As Hickenbotham et al have stated gender, occupation, arm length, solar radiation and refractive error are some of the factors that affect the age of onset of presbyopia.12 Presbyopia starts to become functionally apparent around 40 years old and affects individuals for a considerable part of their working life.
The adoption of digital technology and the internet for social and professional purposes has made near vision a necessity owing to increased screen time. Lack of clear near vision also affects regular reading, office work and manuscript working negatively.13 A study conducted in Nigeria on the quality of life of people aged greater than 40 in 2015 found a decrease in quality of life by 22%14 and another literature review done by Berdahl et al in 2020, stated uncorrected presbyopia has caused a 2-fold increase in difficulty in near vision related activities, and an 8-fold increase in difficulty in very demanding near vision related tasks.3
The only study done on presbyopia in Eritrea was done in 2013, a community based study conducted in Zoba Maekel. It found a prevalence of presbyopia of 32.9% with only 9.9% spectacle coverage. There is no other study in the rest of the country or a newer study showing the current status of presbyopia in Eritrea. But based on the 2013 study, there is a large load of unmet presbyopia requirements.15 The main objective of this study was to determine an age-appropriate presbyopic correction for Asmara inhabitants. The observation of other variables such as age, gender, occupation, refractive error, and finding out the prevalence of presbyopia and other demographic details were sub-objectives of this study.
This was a hospital-based cross-sectional study performed on all patients visiting hospitals during the course of the study. The study population were the inhabitants of Asmara whose population is 613,512, according to a 2013 study of the office of demographics of Asmara. This study was conducted at Biet-Mekae Community Hospital, Godaif Community Hospital and Brhan Ayni Referral Eye Hospital in Asmara from June to September 2017.
Where:
n = sample size; z = 1.96 (with confidence interval 95%);
e = 0.03 (error of acceptance); p = 0.5 (probability of occurrence);
q = (1-p); n = 385
The sample size calculation yielded a sample size of 385, to strengthen the results of the study 1310 participants were included. The sampling procedure was as follows: anyone who visited the hospital during the study period.
The inclusion criteria were living in Asmara, age 35–60 years, a best-corrected visual acuity (VA) of 6/9 or better in both eyes. Participants with anisometropia greater than 1.5 diopter spherical (DS) and binocular vision problems (amblyopia, strabismus, nystagmus or monocular patients) were excluded. Aphakic or pseudophakic participants were also excluded and those with ocular or systemic pathologies that could affect their accommodation or fusional vergence. Patients taking medication that could affect accommodation were excluded.
The following procedures were performed as per the following sequential order on the participants to determine the near addition.
Performa: was used to record the participants’ profile; their age, gender, job, address and examination results. Based on their occupation the participants were classified as office workers, housewives or laborers to provide an idea about their daily sun exposure.
Visual acuity: was measured using ICEE Snellen E chart at 2.5 meters under ambient indoor illumination, both eyes monocularly and the measurement was stopped at 6/6. Near VA was obtained using a LVRC Bailey-Lovie Near chart, it was measured in both eyes monocularly at 40 cm and it was stopped at Log MAR 0.00.
Ocular exam: an anterior segment exam was performed using a Haag Streit slit lamp and the posterior segment exam was performed using Keeler direct ophthalmoscope.
Static dry retinoscopy: was performed in a darkened room with the patient fixating on the distance chart and the working distance lens placed on the trial frame.
Subjective refraction: was performed binocularly with a fogging lens placed on one eye while refraction is done on the other eye. The retinoscopic result was used as the starting point, and the maximum plus that gave the best VA was taken as the end point of refraction. Those with best-corrected monocular VA less than 6/9 were excluded.
Dynamic retinoscopy: the monocular estimation method was used with the results of the subjective refraction on place and Tigrinya letters as target at 40 cm, the customary working distance. The result was used as the baseline for the subjective verification of the near addition after reducing +0.75 DS for lag of accommodation.
Amplitude of accommodation: was measured afterwards using the push-up method with the Royal Air Force (RAF) rule using target of 0.7 Log MAR.
Near addition: the dynamic retinoscopy result was used as a starting point after reducing 0.75 DS for lag of accommodation. Subsequently, subjectively verified until VA of 0.00 Log MAR was reached.
The agreement between the three examiners was evaluated before the start of the study by evaluating the same 5 participants. The study commenced after the examiners agreed in their results to 0.25 DS.
Presbyopia: participants were defined as presbyopic if they were unable to read 20/50 optotype at 40 cm in ambient room illumination with distance correction in place and their VA improved by at least one line with 1 DS.16
Near add: lens power which enabled patients to read the 0.00 Log MAR with the minimum plus at 40 cm.17
The obtained data were entered into SPSS version 20, and various statistical tests were run on the software. For two-by-two variables Fisher’s exact test was performed, for variables with more than two values; however, one-way analysis of variance (ANOVA) was used. Automatic linear progression was performed to determine the effect of the variables on the given addition in terms of their predictive importance. To see the effect of refractive error on the near addition, the participants were regrouped based on their refractive status and one-way ANOVA was run on them. A confidence interval of 95% was taken and a p-value less than 0.05 was considered significant.
Ethical approval was obtained from the Ethics Committee of Asmara College of Health Sciences and Ministry of Health of Eritrea, after they have proved that the study follows the Helsinki Declaration. The ethical committee approved of obtaining an informed verbal consent from the participants prior to the examination.
This study included 1310 participants of whom 48.5% were females and the remaining 51.5% males. It included people of varying occupations who were classified as office workers, laborers and housewives. Table 1 shows the demographic distribution of the participants, and the number of participants who had refraction performed for them previously.
 | Table 1 Demographic Distribution of Participants |
Among those with a previous prescription only 54.3% presented with their glasses, the remaining 45.7% did not have their spectacles. Among those who presented with glasses 19.4% of them had no prescription and were near glasses they bought themselves. There was no significant difference in previous refraction between the two sexes.
Out of the 1310 participants 74.1% were found to be presbyopic and the remaining 25.9% were not yet presbyopic. Table 2 illustrates the percentage of presbyopic people found in the study across genders and occupations.
 | Table 2 Prevalence of Presbyopia in Different Variables |
A multivariable analysis was performed on the variables to observe their association to presbyopia, and Table 3 shows the results of the analysis. As age had the highest level of association to presbyopia, the analysis was performed in two steps. The first one included all the variables and observed their impact on addition, while the second one removed age and observed the association of the other variables with presbyopia.
 | Table 3 Multivariate Analysis of the Factors Affecting Presbyopia Age Adjusted and Non- Adjusted |
Among the different variables observed to be associated with the given addition, only age and sex showed statistically significant association. For every increase in age by one year there was an increased risk of presbyopia by 1.76 times, and males were 0.67 times less likely to develop presbyopia than females of the same age.
The study found that 35.6% of the study participants had a previous glass prescription but only 54.3% of them presented with their glasses. Among those who presented with glasses on, 19.4% of them had no prescription for their glasses, 83.6% of those who presented with glasses they had no prescription for were presbyopic. In the presbyopic population, 40.5% of them had a previous prescription and only 29.8% of the presbyopic had previous glasses on presentation.
The addition was affected by various factors, and factors such as age, gender, occupation affected it more significantly than others. Table 4 shows the addition determined in this study for males and females across all the age groups.
 | Table 4 Addition Table for the Different Genders Across the Age Groups |
Figure 1 illustrates the result of Post Hoc tests which were run on the addition across the age groups and the result showed there was a significant difference in the addition across the different age groups with a p-value of <0.001.
The near addition determined for this population was higher than the addition found in Chandigarh, India and lower than pointer determined for the North American population. This could be due to geographical factors as Miranda stated or genetic and racial differences.Figure 218–20
To see the effect of distance refractive error on the near addition, a post-hoc-Tukey and one-way ANOVA tests were performed. The significance of the difference of the given addition across the different refractive status on one-way ANOVA was that it was significant in the age group of 35–40 years, but as age increased the difference in addition significantly decreased.
Table 5 shows the results of the required addition by the different refractive status and the significance of this variation. The post hoc tests revealed that the given addition was similar across all the refractive status in all age groups except between hyperopia and emmetropia in the 35–40 years age group (p < 0.001) and again in the 41–45 years age group (p = 0.003). The remainder showed that refractive error had no significant effect on the near addition.
 | Table 5 Near Addition to Different Refractive Status |
Logistic regression analysis was performed to determine the influence of different variables on addition. The included variables were age, refractive error, occupation, sex, and amplitude of accommodation (AA), which were assessed to determine their predictive importance. Table 6 shows the result of the logistic regression. Among those variables those that displayed importance values less than 0.005 are not shown in the table. The result showed that age had the highest predictive importance of all other variables (0.774), an increase in age was directly proportional to near addition.
 | Table 6 Predictive Factors for Addition |
In this study, the prevalence of presbyopia was 74.2%, this is significantly higher than similar studies conducted in Brazil (54.7%),21 south India (55.3%),22 Tanzania (62%),23 and Nigeria (30.4%).24 The prevalence was higher with increasing age as shown in Table 3; for every 1-year increase in age there was a 1.785 times risk of developing presbyopia after the age of 35 years, matching the results of a Tanzanian study.16
The prevalence of presbyopia differs according to gender and occupation as demonstrated in Table 2. Among 1310 participants 48.7% were female, out of which 70.2% were presbyopic; in the case of males, they contributed to 51.3% of the total participants and 77.8% of them were presbyopic. This higher prevalence of presbyopia in males observed was different from a Brazilian study that found a higher prevalence in females.21 But this result could be attributed to the fact that the females were younger, with a mean age of 45 years, while the males had an average age of 47 years.
In terms of occupation, prevalence of presbyopia varied again. Laborers had a higher prevalence of presbyopia at 79.5%, followed by office workers among which 73% were presbyopes. The odds ratio were 1 for laborers, 0.628 for office workers, and 0.618 for housewives/unemployed within the same age group. This contradicted a Brazilian study, in which presbyopia prevalence increased with an increasing level of education,21 but the findings of Abdulrhman et al clarifies this stating that by having more exposure to the sun, there is a higher ocular temperature which in turn facilitates presbyopia onset.25
When previous refraction is considered, ie participants who had previous eye exams and glasses prescribed for them, there was no significant association between gender and previous refraction with a p value of 0.8. But there was a significant association of previous refraction with age and occupation having p values respectively 0.001 and 0.019. This shows that increasing age and having office work were strongly associated with the likelihood of having ocular exams and glasses prescribed. There was no significant association with the address of the participants and previous glass prescription.
According to the study results, addition had the strongest association with age (p = 0.00). In Table 6 the logistic regression data shows that age had a predictor importance of 0.774 and the highest value, followed by AA with a predictor importance of 0.199 and the logistic regression had an accuracy of 75.1%. There was a direct relationship of increasing addition with age, with a coefficient of 1.643 in the age group of 35–40 years, later this coefficient decreased. The study result showed that for every five years of age there was an increase in the given addition by 0.4–0.5 DS. This was in line with Duane’s26 and Donder’s27 studies who both worked in European populations stating that AA decreases with age which in turn raises the given addition; in their study groups the age of onset of presbyopia was 45 years. A Bolivian study found that the onset of presbyopia was at 38 years and their AA was lower than Duane’s study group. This variety of AA caused due to geographical difference also resulted in a variety in addition.
The addition power for this population was higher than that determined for the North American population but lower than that reported in Chandigarh, India.18 Figure 2 demonstrates a graphic representation of this variation. This variation could be due to geographic variation, average temperature difference in which the average annual temperature of Chandigarh is 28.9 °C, while Asmara’s temperature is 15.6 °C, as Miranda previously stated that the average temperature had the highest impact on the onset of presbyopia.20
The addition accepted by female participants was higher than males of the same age category, similar to the findings of Andrew et al. This could be due to a shorter working distance preference in females as stated by Hickenbotham et al and their lower AA.
In this study the majority of participants, 636 (48.5%), were emmetropic, 480 (36.6%) were hyperopic, and 194 (14.8%) were myopic. The results showed that there was no statistically significant difference in addition among the different refractive statuses except between emmetropic and hyperopic groups in age groups 35–40 years and 40–45 years.
This study obtained valuable information on presbyopes and examined other variables that may have an impact on presbyopia in an area with scarce similar information. However, the inter-observer difference of 0.25 DS could be a source of imprecision in the results. The results can be used as baseline data for future studies in the region and the stated variables can help renovate clinical presbyopia management and identify patients early by identifying risk factors.
There was an inter-observer difference in the refraction of 0.25 DS, which could have caused a certain discrepancy in the results.
The study has found a high number of uncorrected presbyopes in Asmara, poor adherence to their previously prescribed glasses, and also a high association of presbyopia with the female gender. It has also determined the near-addition table, which will facilitate the management of the high number of uncorrected presbyopes in the city. Therefore, an increased access to affordable glasses and vision programs that target women is advisable in the city. The study showed that there is a significant difference in the required addition for different populations owing to various environmental and genetic factors, therefore determination of addition, primarily in areas identified with high number of uncorrected presbyopes, is a prudent step.
AA, amplitude of accommodation; DS, diopter spherical; MAR, minimum angle of resolution; MEM, monocular estimation method; RAF, Royal Air Force; VA, visual acuity.
The data-set supporting the findings of this article is available from the corresponding authors.
Ethical approval for the study was issued from the Eritrean Ministry of Health.
The authors thank the clinical staff who supported this work at Brhan Ayni National Eye Referral Hospital, Biet Mekae Community Hospital and Godaif Community Hospital.
All authors made a significant contribution to the work reported whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Data were collected from the above-mentioned hospitals with no incentive or financial support from any organization.
The authors declare that they have no competing interests.
1. GBD 2019 Blindness and Vision Impairment Collaborators. Trends in prevalence of blindness and distance and near vision impairment over 30 years: an analysis for the global burden of disease study. Lancet Glob Health. 2020. doi:10.1016/S2214-109X(20)30425-3
2. Fricke TR, Tahhan N, Resnikoff S, et al. Global prevalence of presbyopia and vision. Am Acad Ophthalmol. 2018;125(0161–6420/18):1492–1499. doi:10.1016/j.ophtha.2018.04.013
3. Berdahl J, Bala C, Dhariwal M, et al. Patient and economic burden of presbyopia: a systematic literature review. Clin Ophthalmol. 2020;14:3439–3450. doi:10.2147/OPTH.S269597
4. Hookway LA, Frazier M, Rivera N, Ramson P, Carballo L, Naidoo K. Population-based study of presbyopia in Nicaragua. Clin Exp Optom. 2016;99(6):559–563. doi:10.1111/cxo.12402
5. Holden BA, Fricke TR, Ho SM, et al. Global vision impairment due to uncorrected presbyopia. Arch Ophthalmol. 2008;126(12):1731–1739. doi:10.1001/archopht.126.12.1731
6. Malhotra S, Vashist P, Kalaivani M, et al. Prevalence and causes of visual impairment amongst older adults in a rural area of North India: a cross-sectional study. BMJ Open. 2018;8(3):e018894. doi:10.1136/bmjopen-2017-018894
7. Idowu OO, Aribaba OT, Onakoya AO, Rotimi-Samuel A, Musa KO, Akinsola FB. Presbyopia and near spectacle correction coverage among public school teachers in Ifo Township, Southwest Nigeria. Niger Postgrad Med J. 2016;23(132):6. doi:10.4103/1117-1936.190342
8. Berhanu Andualem H, Assefa N, Weldemichael D, et al. 2017 Prevalence and associated factors of presbyopia among school teachers in Gondar city, Northwest Ethiopia. Clin Optom. 2016;9:85–90. doi:10.2147/OPTO.S129326
9. Kumah D, Lartey S, Amoah-Duah K. Presbyopia among public senior high school teachers in the Kumasi metropolis. Ghana Med J. 2011;45(1):27–30. doi:10.4314/gmj.v45i1.68919
10. American Optometric Association. Optometric clinical practice guideline care of the patient with presbyopia; 2010. Available from: https://www.aoa.org/documents/optometrists/CPG-17.pdf. Accessed September 1, 2023.
11. Goertz AD, Stewart WC, Burns WR, Stewart JA, Nelson LA. Review of the impact of presbyopia on quality of life in the developing and developed world. Acta Ophthalmol. 2014;92(6):497–500. doi:10.1111/aos.12308
12. Hickenbotham A, Roorda A, Steinmaus C, et al. Meta-analysis of sex differences in Presbyopia. Investig Ophthalmol Vis Sci. 2012;53:3215–3220. doi:10.1167/iovs.12-9791
13. Reddy PA, Congdon N, Mackenzie G, et al. Effect of providing near glasses on productivity among rural Indian tea workers with presbyopia (PROSPER): a randomized trial. Lancet Glob Health. 2018;6(9):E1019–E1027. doi:10.1016/S2214-109X(18)30329-2
14. Munaw MB, Kebede BN, Adimassu NF, et al. Unmet need for presbyopia correction and its associated factors among school teachers in Hawassa city, South Ethiopia. BMC Ophthalmol. 2020;20(1):188. doi:10.1186/s12886-020-01454-5
15. Muhammad N, Alhassan MB, Umar MM. Visual function and vision-related quality of life in presbyopic adult population of North western Nigeria. Niger Med J. 2015;56(5):317–322. doi:10.4103/0300-1652.170379
16. Fai Chan V, Mebrahtu G, Ramson P, et al. Prevalence of refractive error and spectacle. Ophthalmic Epidemiol. 2013;20(3):131–137. doi:10.3109/09286586.2013.783082
17. Burke AG, Patel I, Munoz B, et al. 2005 Population-Based Study of Presbyopia in rural Tanzania. Am Acad Ophthalmol. 2066;113(5):723–727. doi:10.1016/j.ophtha.2006.01.030
18. Jain IS, G JRA, Gupta A. Early onset of Presbyopia. Am J Optom Physiol Opt. 1982;59(12):1002–1004. doi:10.1097/00006324-198212000-00012
19. Pointer JS. The presbyopic add, II: age-related trend and a gender difference. Ophthalmic Physiol Opt. 1995;15(4):241–248. doi:10.1046/j.1475-1313.1995.9400022r.x
20. Miranda MN. The geographic factor in the onset of presbyopia. Am Ophthalmol. 1979;87(5):666–669.
21. Duarte WR, Barros AJ, Dias-da-Costa JS, Cattan JM. Prevalência de deficiência visual de perto e fatores associados: um estudo de base populacional [Prevalence of near vision deficiency and related factors: a population based study in Brazil]. Cad Saude Publica. 2003;19(2):551–559. Portuguese. doi:10.1590/S0102-311X2003000200022
22. Nirmalan PK, Krishnaiah S, Shamanna BR, Rao GN, Thomas R. A population-based assessment of presbyopia in the state of Andhra Pradesh, south India: the Andhra Pradesh eye disease study. Invest Ophthalmol Vis Sci. 2006;47(6):2324–2328. doi:10.1167/iovs.05-1192
23. Patel I, Munoz B, Burke AG. Impact of presbyopia on quality of life in a rural African setting. Ophthalmology. 2006;113(5):728–734. doi:10.1016/j.ophtha.2006.01.028
24. Umar MM, Muhammad N, Alhassan MB. Prevalence of presbyopia and spectacle correction coverage in a rural population of North West Nigeria. Clin Ophthalmol. 2015;9:1195–1201. doi:10.2147/OPTH.S81194
25. Abdulrhman A, Cotlier E. Effect of sunlight and ambient temperature on the lens and aqueous humor: observations in New Haven, Conn, and Chandigarh India. ARVO Abstr. 1980;1980:65.
26. Duane A. Normal values of the accommodation at all ages. JAMA. 1912;59(12):1010–1013. doi:10.1001/jama.1912.04270090254042
27. Donders FC. On the Anomalies of Accommodation and Refraction of the Eye. London: The New Sydenham Society; 1864:206–211.
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License. By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License. By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.



